Self-Recognition and Self-Preference Regarding Facial Profile and Its Association with A-Point–Nasion–B-Point (ANB) Angle in Orthodontic Patients
By Ahsan Mehmood Shah, Mashal AfridiAffiliations
doi: 10.29271/jcpsp.2024.03.318ABSTRACT
Objective: To detect any association between the A-Point-Nasion-B-Point angle, self-recognition and self-preference, and to find the association of these variables with the skeletal class, age, and gender.
Study Design: Cross-sectional study.
Place and Duration of the Study: Department of Orthodontics and Dentofacial Orthopaedics, Khyber College of Dentistry, from October 2022 to April 2023.
Methodology: A right-sided profile photograph of each participant was taken, and the lower jaw was moved 5mm backward and forward to produce 2 alterations. The participants were shown their 3 photographs, from which they picked the one they perceived to be their original photograph and the one they preferred for themselves. Chi-square tests for association and binary logistic regression were employed to find the associations between the variables. The alpha value was 0.05.
Results: Ninety-eight male and 109 female orthodontic patients, mean age of 17.08 + 4.78 years, were recruited. A significant proportion of participants (51.2%) correctly identified themselves. Every degree increase in ∠ANB reduced the odds of correct self-recognition, and of self-preference for the original profile, by 1.1. There was self-preference for that profile which the participants believed was the original (57%). Skeletal class III were less likely to prefer a protrusive profile (p = 0.005). Patients aged between 15 to 22 years were able to correctly identify their profiles (63.9%, p <0.001).
Conclusion: There is an association between facial profile self-recognition and self-preference. The ∠ANB negatively relates to self recognition. An increase in ∠ANB reduces self-preference for the original profile.
Key Words: Cephalometry, Dental photography, Self-perception, Corrective orthodontics.
INTRODUCTION
Orthodontics is primarily oriented towards correcting abnormal tooth positions and occlusion. Most people seek orthodontic treatment to improve their facial appearance.1 The profile is the right side of the face, observed at 90° from the front. What constitutes a beautiful, profile differs among racial groups.2-4 Hence, determining the community’s local norms and correlating them with the patient’s opinion, who is the major stakeholder in treatment, should not be overlooked as facial aesthetics may be impacted by the decisions of the orthodontist through the treatment they provide.
In recent decades, patient satisfaction has increased as a result of orthodontists starting to value patients' opinions more recently.5 Yet still, many orthodontists are focused on achieving a class I skeletal and dental relationship because they are academically trained to believe that class I relationships are the most pleasing ones,6 although studies show that laypeople are mostly unaware of their own profiles,6 and are less critical and more forgiving towards class II and class III relationships of others.7-9
According to an Italian study, patients are familiar with their frontal view, but are unaware of their profile view.10 After exposure to photographs of their profile views, 45% participants were willing to undergo orthodontic treatment to change their facial appearance. A recent Pakistani survey found that 50% people between 20-30 years were willing to undergo orthodontic therapy only for aesthetic improvement.11 Studies show that adolescents between 15-25 years are more likely to be aware of their profiles.12,13 In studies carried out to assess whether patients are familiar with their profiles, silhouettes were used, despite silhouettes not being good indicators of anteroposterior jaw positions.14 To the author’s knowledge, no study since 199915 altered the patients’ profile photographs and exposed them to the altered versions to record their opinion, and no study has attempted to find an association of A-Point–Nasion–B-Point angle (∠ANB) with self-recognition and self-preference.
Detection of unawareness, misperception or displeasure a patient may have regarding their profile and knowing which profile they prefer for themselves is crucial before initiating any dentofacial treatment, as it guides the path taken when counselling, performing a Visual Treatment Objective (VTO) and, ultimately, the route of treatment – orthopaedic, orthodontic, orthognathic. This study’s primary aim was to determine whether individuals can identify themselves from their profile view (self-recognition), and whether these is any association between ∠ANB, self-recognition and self-preference. Secondary aims were: to ascertain whether skeletal class, age or gender influenced self-recognition; and whether these variables influenced the profile preference a person had for themselves (self-preference).
METHODOLOGY
This cross-sectional study was conducted in the Orthodontics and Dentofacial Orthopaedics Department of Khyber College of Dentistry, from October 2022 to April 2023, after obtaining ethical approval from research review board. The sample size (207) was calculated by using OpenEpi, taking 84% orthodontic patients correctly identified their profiles,16 with 5% margin for error, and 95% confidence interval. Convenience sampling was used to recruit patients undergoing orthodontic treatment. The patients who had undergone orthognathic surgery, had facial asymmetries greater than 5mm, had facial trauma or syndromes affecting facial morphology, and those with a beard were excluded. They patients were informed of the research and written consent was taken.
A right-sided profile photograph of the participant was taken using a Canon 650D DSLR and a Sigma 105mm macrolens, with the patient maintaining a natural head position. The distance between the photographer and the participant was 2.6 metres, with the areas marked on the ground. A scale was held near the participant’s face for calibration parallel to the nose. This photograph was altered using Adobe Photoshop CS6 Extended. The chin was moved 5mm backwards in alter A, with the lip slightly following to maintain a natural appearance. They were similarly moved 5mm forward in alter B (Figure 1).
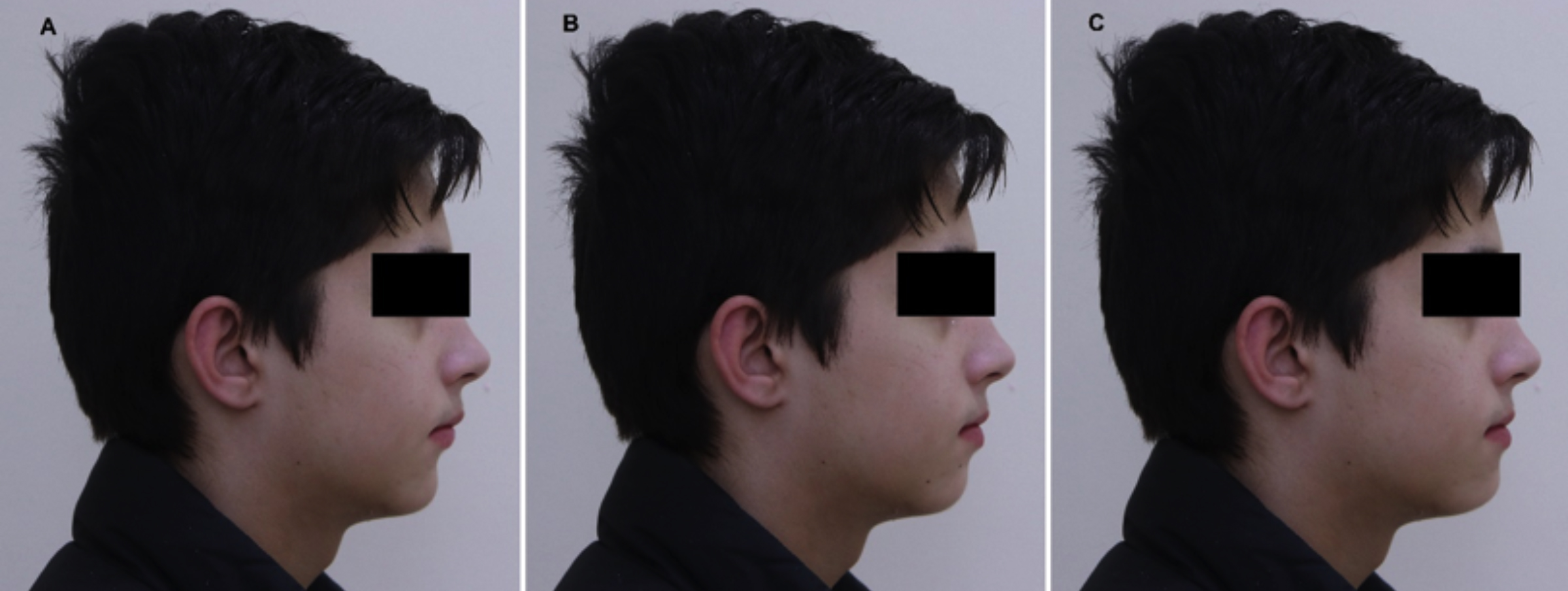 Figure 1: (A) Alter A with a retrusive chin. (B) Original photograph. (C) Alter B with a protrusive chin.
Figure 1: (A) Alter A with a retrusive chin. (B) Original photograph. (C) Alter B with a protrusive chin.
Participants were shown the photographs on a screen in the order; alter A, original photograph, and alter B. They were allowed to move back and forth between the photographs using a controller. They were informed that the difference in the photographs lay only in the lower face. The researcher was present during the process to remove any confusion the participant may have had regarding the procedure, and to make sure that the participant was shuttling between the images, while maintaining a distance to ensure that their presence did not influence the results. The researcher asked the participant to identify which photograph among the three photographs was their original and which they preferred for themselves. The responses were recorded.
Participants’ lateral cephalograms were traced on an acetate sheet. Sella, Nasion, A-Point and B-Point landmarks were traced. ∠SNA and ∠SNB were drawn, and ∠ANB was calculated. Skeletal class was determined using ∠ANB, into class I (∠ANB: 2-4), class II (∠ANB: >4), and class III (∠ANB: <2). After 2 months, selected cephalograms were re-traced to check for intra-observer reproducibility using Intra-class Correlation Coefficient. It was found to be 0.89, which is considered excellent.
Grouping with respect to self-recognition was done. Those participants who correctly identified themselves were categorised into the self-recognising (SR) group; those who failed to identify themselves correctly were categorised into the non-self-recognising (NSR) group. NSR was further divided into NSR-A (those who identified themselves as alter A) and NSR-B (those who identified themselves as alter B).
Grouping with respect to age: Group A: <15 years, Group B: 15 to 22 years, Group C: >22 years. Data were analysed using SPSS 25. Categorical variables of gender, age group, skeletal class, self-recognition, and self-preference are presented as frequency and percentage. Numeric variables of age and ∠ANB are presented as mean with standard deviation (SD). Binary logistic regression was used, at alpha 0.05, to find the effect of ∠ANB on self-recognition and self-preference. The odds ratios were determined to see how an increase/decrease in the ∠ANB would increase/decrease the probability that participants would recognise themselves, and would prefer their original profiles.
Chi-Square test for association, at alpha 0.05, determined whether there was any association between self-recognition and self-preference, and between self-recognition/self-preference and skeletal class, age group, and gender. When an association was found, a chi-square post-hoc17 test was applied to determine which combinations were significant (adjusted alpha values 0.008 and 0.005).
RESULTS
There were 98 (47.3%) males and 109 (52.7%) females. Age ranged from 8-30 years, mean age 17.08 + 4.78 years. The mean age of males was 16.84 ± 4.56 years and for females, it was 17.29 ± 4.98 years (Table I).
Table I: Demographics of participants.
|
Demographics with respect to self-recognition groups |
|||||||
|
Age Group |
N (%) |
Mean Age (years) |
SD |
Males (%) |
Females (%) |
SR (%) |
NSR (%) |
|
A |
80 (38.6) |
12.64 |
1.46 |
38 (47.5) |
42 (52.5) |
32 (15.5) |
48 (23.2) |
|
B |
97 (46.9) |
18.09 |
2.35 |
48 (49.5) |
49 (50.5) |
62 (30.0) * |
35 (16.9)* |
|
C |
30 (14.5) |
25.63 |
2.14 |
12 (40) |
18 (60) |
12 (5.8) |
18 (8.7) |
|
Total |
207 (100) |
17.08 |
4.78 |
98 (47.3) |
109 (52.7) |
106 (51.2) |
101 (48.8) |
|
*=significant at alpha 0.008 (chi-square post-hoc). |
|||||||
Among the NSRs, 44 (21.3%) identified as NSR-A, whilst 57 (27.5%) as NSR-B. More participants had self-preference for an alter (n=37, 17.9% for alter A; n=85, 41.1% for alter B) over the original profile (n=85, 41.1%).
∠ANB ranged from -7° to 12°. There were 71 (34.3%) participants with skeletal class I, 104 (50.2%) with class II, and 32 (15.5%) with class III.
Logistic regression models were statistically significant. For 1° increase in ∠ANB, the odds of misidentifying one’s profile increased by 1.1 (p=0.046, CI 95%: 1.0 - 1.2), and the odds of preferring an alter over the original profile increased by 1.1 (p=0.023, CI 95%: 1.0 - 1.2).
A moderate association (Cramer’s V: 0.343) between self-recognition and self-preference was found (p<0.001), confirmed by chi-square post-hoc (alpha=0.005), with self-preference for that profile which the participant believed was the original (adjusted <0 .001), at a concordance of 57%. SR were significantly less likely to prefer a more protrusive profile (adjusted p=0.003), while NSR-B were less likely to prefer the original profile (adjusted p=0.001, Figure 2).
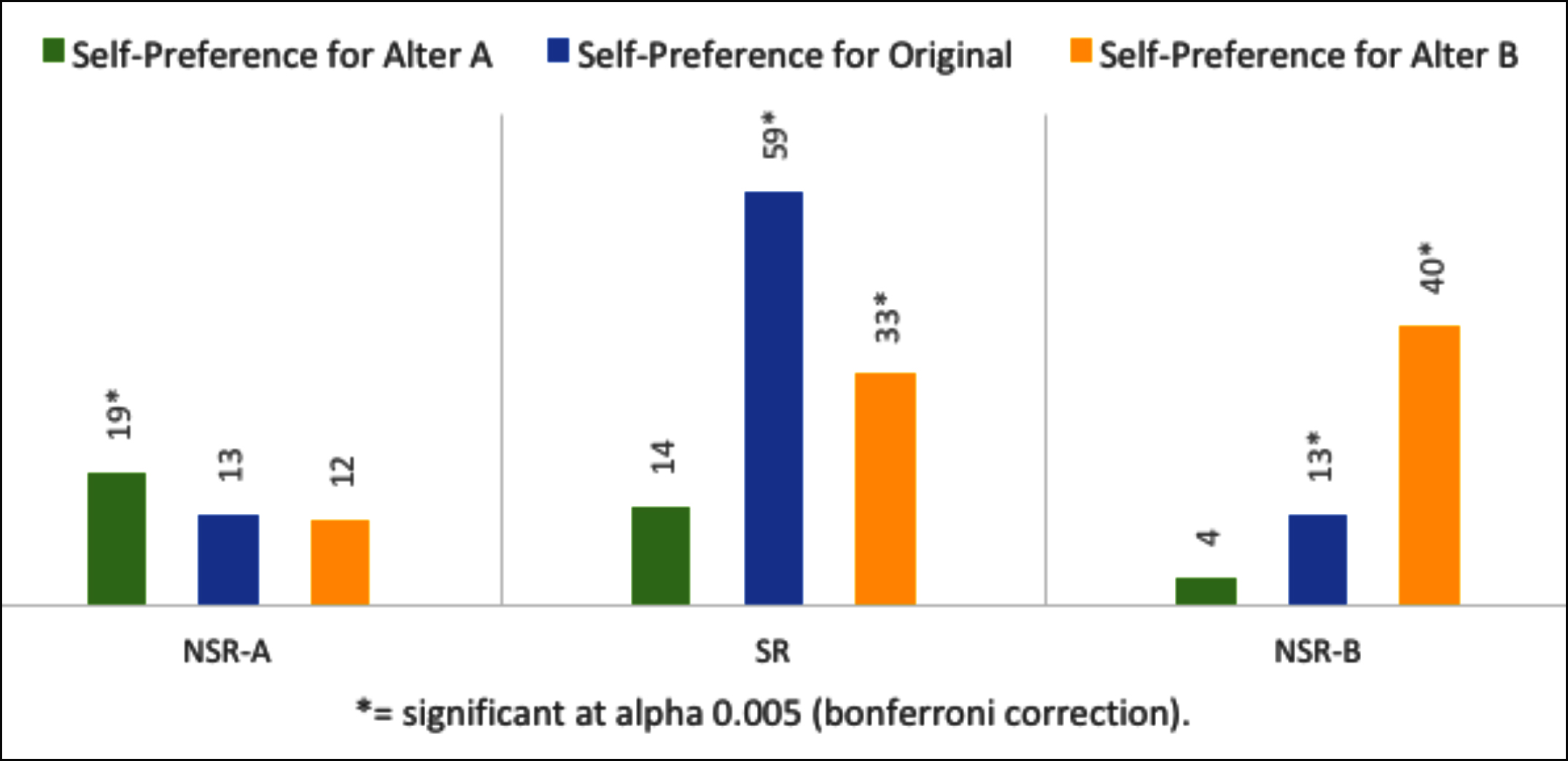 Figure 2: Chi-square test for association between self-recognition with self-preference.
Figure 2: Chi-square test for association between self-recognition with self-preference.
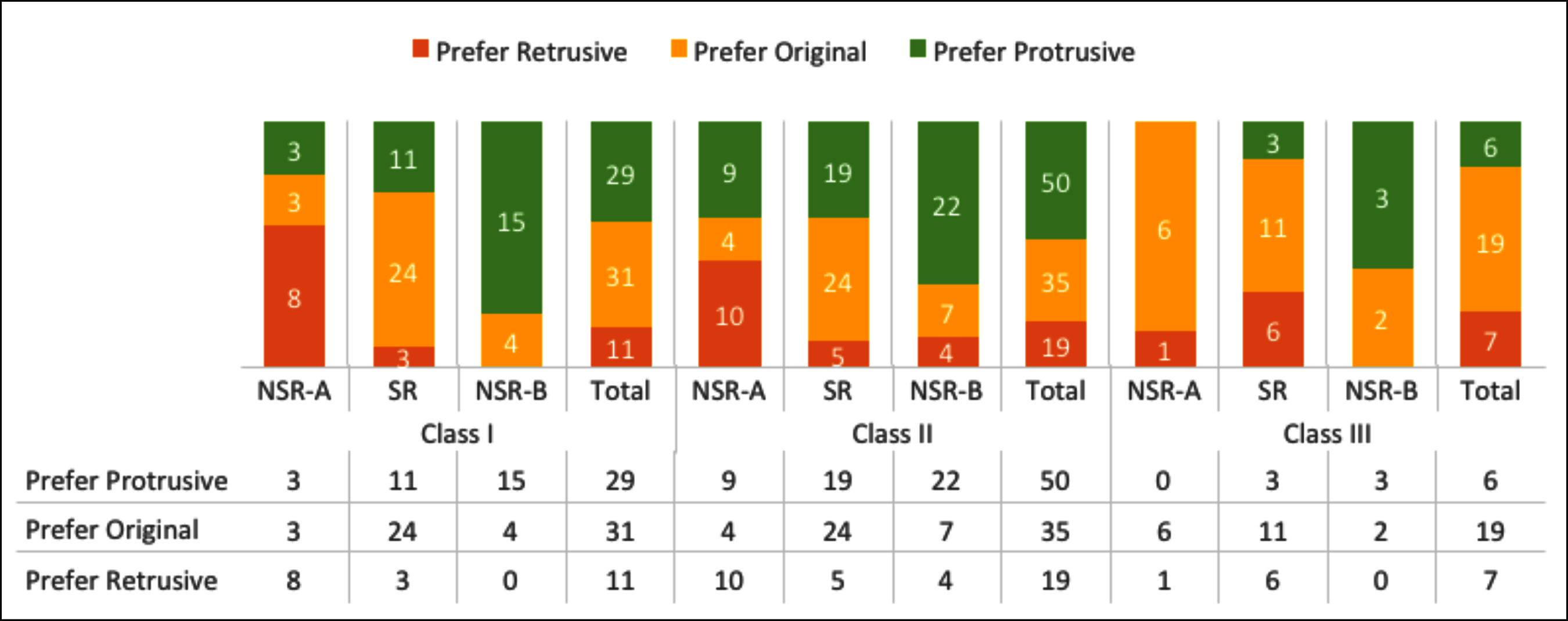 Figure 3: Trends of self-recognition and self-preference among skeletal classes.
Figure 3: Trends of self-recognition and self-preference among skeletal classes.
A weak association (Cramer’s V: 0.154) was found between skeletal class and self-preference (p=0.045), with skeletal class III having reduced self-preference for protrusive profiles (adjusted p=0.005, Figure 3). No association was found between skeletal class and self-recognition (p-value 0.428).
There was a moderate association (Cramer’s V = 0.239) between age and self-recognition (p = 0 .003), confirmed by chi-square post-hoc (alpha = 0.008). Group B recognised their profiles (p = <.001) with self-recognition rate of 63.9% (Table I). Age did not influence self-preference (p = 0.992). There was no association between gender and self-recognition (p-value 0.058) or self-preference (p = 0.288).
DISCUSSION
A number of studies have been done to ascertain whether there is any difference between the aesthetic perception of orthodontists, orthodontic patients, maxillofacial surgeons, dental students and laypeople.8,18 This study focuses on the primary stakeholders of orthopaedic/orthodontic therapy and orthognathic surgeries – the patient. This study differs from others as instead of silhouettes, the patients’ photographs were modified and an association with ∠ANB was found.
In this study, 50% patients correctly identified themselves. This compares well with the recognition rate by Eslami et al.,19 at 64.9% among orthodontic patients above 13 years of age. Although, Sharma et al.16 concluded it to be higher - 84% among 14-22-year.
As ∠ANB increased - hence the anteroposterior distance between the jaws increased - self-recognition decreased. This may be because laypeople generally assume that they carry a near straight profile.6 People with skeletal class I and class III, with smaller ∠ANB values, have straighter profiles, so are more likely to correctly guess their profiles compared to skeletal class II people with rounded profiles.
As ∠ANB increased, and the profile moved from straighter to rounder, preference for a protrusive, hence, straighter profile increased. A greater ∠ANB indicates a skeletal class II, and thus, a retrusive chin, which laypeople consider unesthetic.20 No previous study with ∠ANB was found for comparison.
Participants preferred that profile for themselves which they perceived was the original - satisfaction rate of 57%. A similar rate (61.9%) was found by Ryan et al. among 15-55 years.13 Zulfiqar et al. and Pace et al. found that a normal profile was most preferred and a retrusive one was disliked.2,8 In this study, a retrusive profile was preferred if one believed it was the original.
Skeletal class had no association with self-recognition and a weak one with self-preference. Volpato et al. similarly concluded that profile convexity did not affect pleasantness scores assigned by patients to themselves.7 In contrast, Eslami et al. found that straight skeletal class I patients rated themselves higher, whereas the other two skeletal classes rated themselves lower, among 13-18-year.19
There were three age groups, partially based on the findings of Varatharaju et al. that adolescents above 15 years had higher self-recognition compared to younger individuals.12 This was supported in this study, in which 15-22-year were better at self-recognition. Although this ability was lost as they entered the adult years of 23 and above. An explanation may be that the 15 to 22 years age window includes the teenage years, when social acceptance and appearance are paramount. Peers are more likely to point out flaws, consequently, adolescents are aware of their imperfections, and thus, can identify themselves.21 As they enter the tougher years of life, only the frontal view still holds importance.22 Bullen et al.’s study on lip procumbrance also supported that 15-25 year could recognise their profile silhouettes, and those above 25 years could not.13 Sharma et al. conducted a study on 14-22 year and found a very high self-recognition rate of 84% among orthodontic patients.16
In this study, gender had no role in determining self-recognition or self-preference. Volpato et al. also found gender to have no role among 15-55 year.7 This contrasts to the findings of the Varatharaju et al. that females had higher self-recognition.12
Having knowledge of the patient’s awareness and prefe-rence regarding their profile before initiating treatment is crucial. People are most likely to prefer that profile for themselves which they believe to be their original one, which indicates that most people are satisfied with their assumed profiles, and hence, may not be eager to change it on the recommendation of the treating doctor. In young patients undergoing orthopaedic treatment, this may determine compliance. If a patient assumes they have a ‘normal’ profile, simply encouraging them to wear their appliance to improve jaw relationships will prove unsuccessful as they may feel that they do not need any improvement. Similarly, if a VTO is performed and the patient does not prefer the new profile, they will be discouraged from wearing the appliance, producing a reverse of the intended effect. It is advised to first ascertain a child’s preference and follow this with a VTO if it favours compliance, or skip it if it discourages compliance.
For adult patients, it should never be assumed that they are aware of an existing jaw discrepancy and prefer correcting it. The patient’s expectations from treatment must be known before treatment planning and should guide the treatment plan. For patients with a jaw discrepancy, ascertain whether they are aware of it (self-recognition), and how willing they are to correct it (self-preference). They should be educated regarding the pros and cons of camouflage and surgery. Perform a VTO and then guide the patient along the treatment path, instead of enforcing a treatment plan on an unwilling patient on the grounds of ‘in the best interests of the patient’.
This study focused on chin movements. The maxilla and vertical growth patterns were disregarded, even though they may influence the results.14,19 Future studies should devise a questionnaire to find out why people favour particular profiles. This may explain their choices. This study had a very large proportion of skeletal class II patients and a small number of cases in group C. It is recommended for future studies that a comparison between the skeletal classes be carried out with equal participants in each group.
CONCLUSION
Half of the orthodontic patient population correctly identified their profiles, with 15-22-year better at self-recognition. Most preferred that profile for themselves which they believed was the actual one. As the ∠ANB increased, the patients were less likely to recognise their original profile and also less likely to prefer it for themselves. Gender did not influence self-recognition or self-preference.
ETHICAL APPROVAL:
The research work was initiated after ethical approval was granted by the Research Review Board of the hospital.
PATIENT’S CONSENT:
All patients were informed that their data will be published for research work. They gave consent for publishing of the data.
COMPETING INTEREST:
The authors declared no conflict of interest.
AUTHORS’ CONTRIBUTION:
AMS: Conception and design of the research, revising it critically for important intellectual content.
MA: Designing of the research, data collection, statistical analysis, interpretation of data, and drafting of the manuscript.
Both authors approved the final version of the manuscript to be published.
REFERENCES
- Prado LH, Previato K, Delgado RZR, Nelson Filho P, Bezerra Segato RA, Nakane Matsumoto MA, et al. Adolescents’ perception of malocclusion, their motivations, and expectations concerning the orthodontic treatment. Is it all about attractiveness? A qualitative study. Am J Orthod Dentofacial Orthop 2022; 161(4):e345-52. doi: 10.1016/j. ajodo.2021.10.014.
- Zulfiqar K, Bahir U KO. Assessment of the most preferred facial profile amongst patients and Orthodontists. Pakistan Orthod J 2013; 5(2):38-43.
- Romsics L, Segatto A, Boa K, Becsei R, Rózsa N, Párkányi L, et al. Patterns of Facial Profile Preference in a Large Sample of Dental Students: A Cross-Sectional Study. Int J Environ Res Public Health 2021; 18(16):8554. doi: 10.3390/ijerph 18168554.
- Imani MM, Sanei E, Niaki EA, Shahroudi AS. Esthetic preferences of orthodontists, oral surgeons, and laypersons for Persian facial profiles. Am J Orthod Dentofac Orthop 2018; 154(3):412-20. doi: 10.1016/j.ajodo.2017.11.040.
- Shelswell J, Patel VA, Barber S. The effectiveness of interventions to increase patient involvement in decision-making in orthodontics: A systematic review. J Orthod 2022; 49(2):129-42. doi: 10.1177/14653125211048202.
- Al Taki A, Guidoum A. Facial profile preferences, self-awareness and perception among groups of people in the United Arab Emirates. J Orthod Sci 2014; 3(2):55-61. doi: 10.4103/2278-0203.132921.
- Volpato GH, de Almeida-Pedrin RR, Oltramari PVP, Freire Fernandes TM, de Almeida MR, de Castro Ferreira Conti AC. Self-perception of facial esthetics by patients with different profiles compared with assessments of orthodontists and lay people. Am J Orthod Dentofacial Orthop 2020; 158(6):840-8. doi: 10.1016/j.ajodo.2019.10.027.
- Pace M, Cioffi I, D’antò V, Valletta A, Valletta R, Amato M. Facial attractiveness of skeletal class I and class II malocclusion as perceived by laypeople, patients and clinicians. Minerva Stomatol 2018; 67(3):77-85. doi: 10.23736/S0026-4970.18.04111-0.
- Fabré M, Mossaz C, Christou P, Kiliaridis S. Orthodontists’ and laypersons’ aesthetic assessment of Class III subjects referred for orthognathic surgery. Eur J Orthod 2009; 31(4):443-8. doi: 10.1093/ejo/cjp002.
- Bonetti GA, Alberti A, Sartini C, Parenti SI. Patients’ self-perception of dentofacial attractiveness before and after exposure to facial photographs. Angle Orthod 2011; 81(3):517-24. doi: 10.2319/101510-606.1.
- Ilyas Muhammad, Shaheen A, Amjad S, Zubair T, Tariq A. Comparison of knowledge and perception of orthodontic treatment among dental students and local population. Saudi J Oral Dent Res 2021; 6(1):59-62. doi:10.36348/ sjodr.2021.v06i01.012.
- Varatharaju V, Caflisch M, Soroken C, Kiliaridis S, Anto-narakis GS. Does age influence self-perception of the soft-tissue profile in children? Am J Orthod Dentofac Orthop 2021; 159(3):e207-15. doi: 10.1016/j.ajodo.2020.10.016.
- Bullen RN, Kook YA, Kim K, Park JH. Self-Perception of the Facial Profile: An Aid in Treatment Planning for Orthognathic Surgery. J Oral Maxillofac Surg 2014; 72(4):773-8. doi: 10.1016/j.joms.2013.09.015.
- Schwabe SA, Caldwell S. Can anteroposterior skeletal pattern be determined from a silhouetted profile photo-graph? A cross-sectional study. J Orthod 2022; 49(1):48-55. doi: 10.1177/14653125211028862.
- Kitay D, BeGole EA, Evans CA, Giddon DB. Computer-animated comparison of self-perception with actual profiles of orthodontic and nonorthodontic subjects. Int J Adult Orthodon Orthognath Surg 1999; 14(2):125-34.
- Sharma S, Trehan M, Naqvi ZA. Perception of facial profile: How you feel about yourself. Int J Clin Pediatr Dent 2011; 4(2):109-11. doi: 10.5005/jp-journals-10005-1092.
- Beasley TM, Schumacher RE. Multiple Regression Approach to Analyzing Contingency Tables: Post Hoc and Planned Comparison Procedures. J Exp Educ 1995; 64(1):79-93. doi:10.1080/00220973.1995.9943797.
- de Sena LMF, Damasceno e Araújo LAL, Farias ACR, Pereira HSG. The influence of sagittal position of the mandible in facial attractiveness and social perception. Dental Press J Orthod 2017; 22(2):77-86. doi: 10.1590/2177-6709.22.2. 077-086.oar.
- Eslami N, Omidkhoda M, Shafaee H, Mozhdehifard M. Comparison of esthetics perception and satisfaction of facial profile among male adolescents and adults with different profiles. J Orthod Sci 2016; 5(2):47-51. doi: 10.4103/2278- 0203.179406.
- Salehi P, Azadeh N, Beigi N, Farzin M. Influence of Age on Perception of Best Esthetical Profile. J Dent (Shiraz, Iran) 2019; 20(1):16-23. doi: 10.30476/DENTJODS.2019.44558.
- Morales-Salazar SA, Monteagudo-Sangama JM, Arriola-Guillén LE. Influence of dentofacial characteristics on the appearance of self-reported bullying: A review. Dent Med Probl 2022; 59(4):657-61. doi: 10.17219/dmp/138636.
- Ishii LE, Nellis JC, Boahene KD, Byrne P, Ishii M. The Importance and Psychology of Facial Expression. Otolaryngol Clin North Am 2018; 51(6):1011-7. doi: 10. 1016/j.otc.2018.07.001.